Most facilities still navigate accreditation with spreadsheets and manual document compilation. Regain reads facility EMR data via FHIR R4 and evaluates it against published Standards continuously, as care happens. Roughly 85% of routine compliance checks automate; the rest stays with the reviewer.
Standards as versioned rule packs.
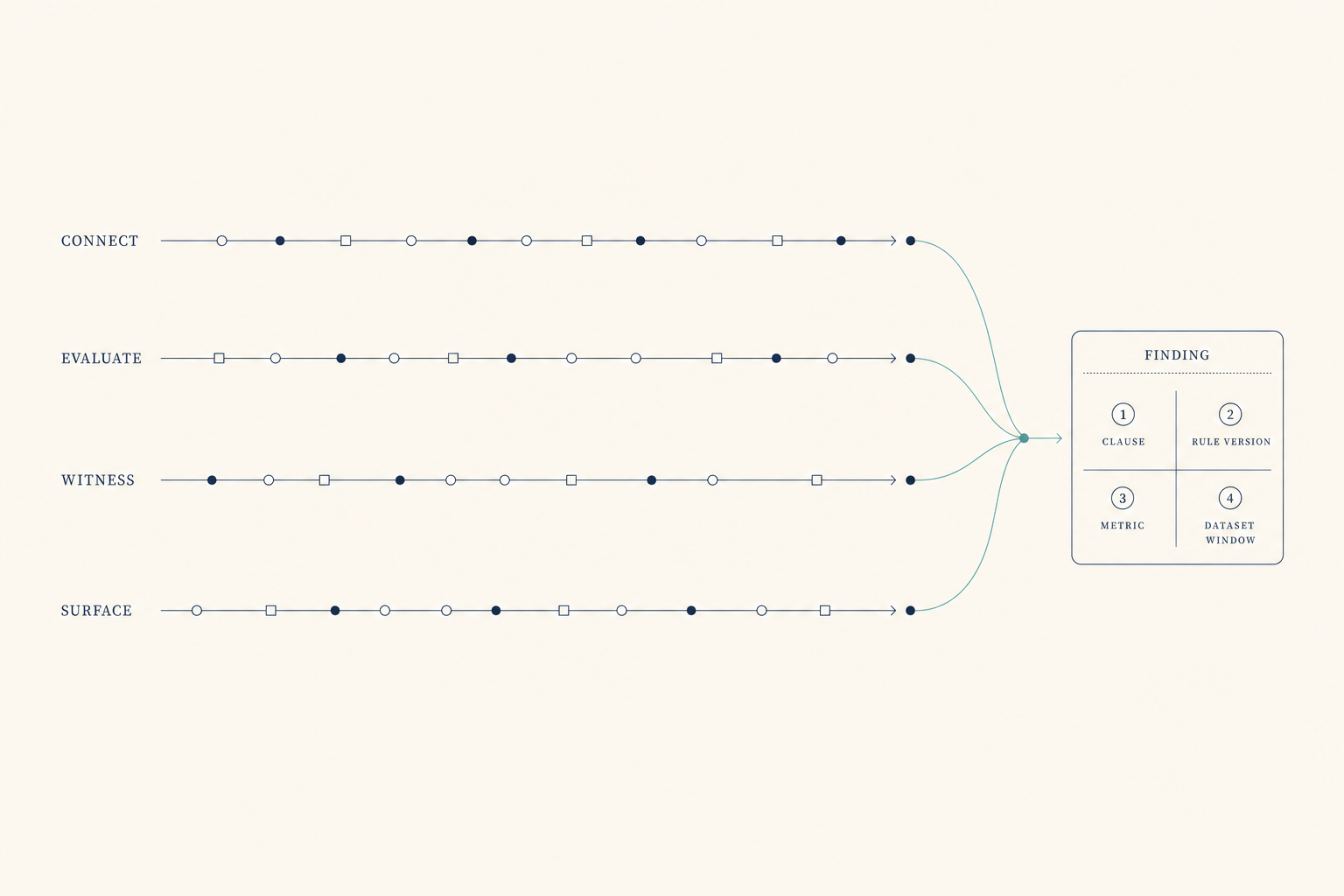
64 rules drawn from a published 2025 echo accreditation Standards document. Each finding cites a clause, a rule version, a metric, and a dataset window.
Evidence as continuous flow.
Clinical data is evaluated deterministically as care happens.
One loop, two readings.
The same connection that evaluates a facility against published Standards also surfaces how clinical AI is used in practice. Override patterns and AI-vs-final-reading concordance accrue to the accrediting body by the structure of the relationship.
Standards authority unchanged.
The pipeline executes published Standards, never authors them. Peer review and the accreditation decision stay with the accrediting body.
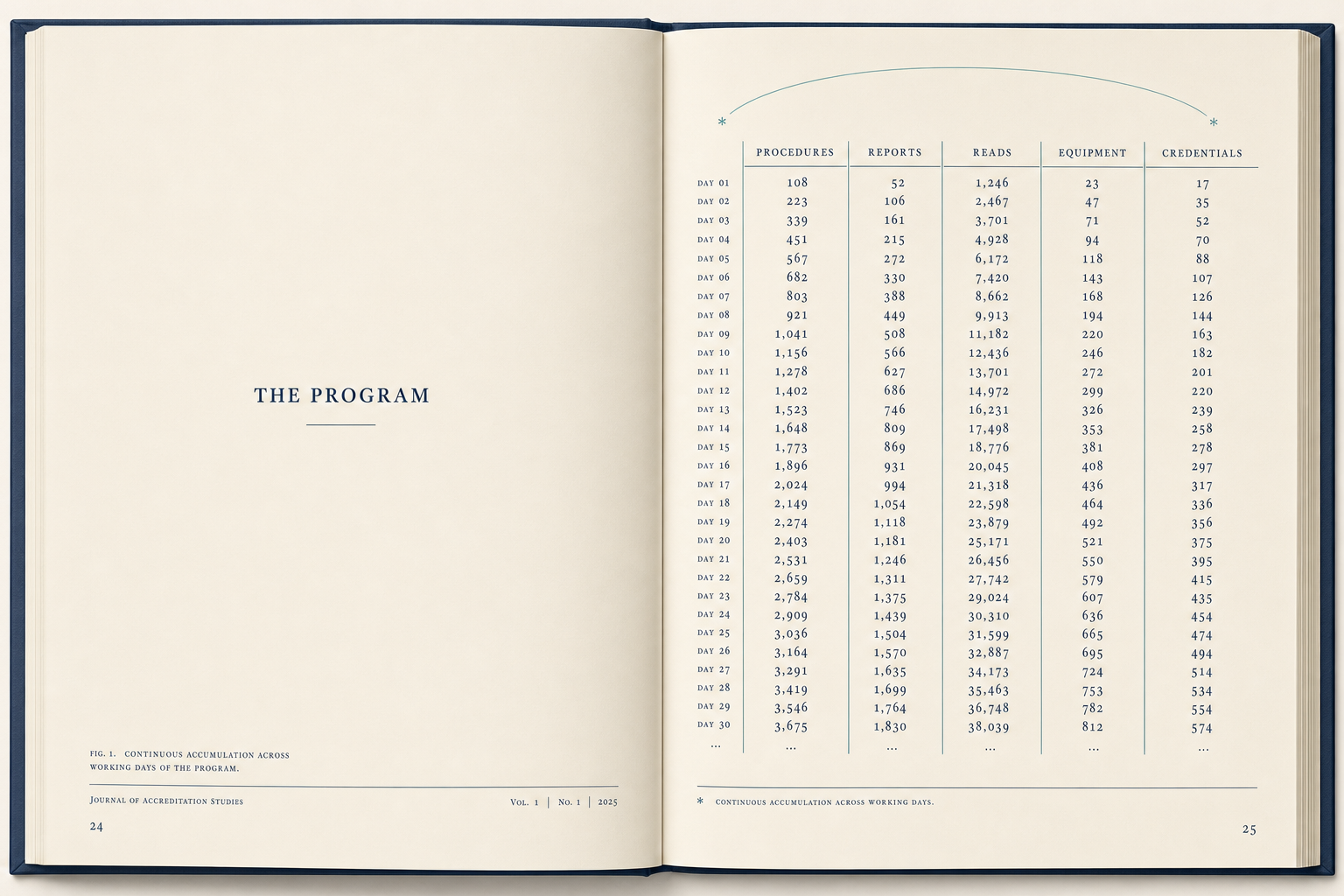
A program. A set of Standards. A three-year cycle. And the gap in between.
01
The Program
A modality program inside a facility runs procedures, writes reports, captures reads, services equipment, and renews credentials at volume, every working day, year after year. Each of those procedures, reports, and reads is evidence, for or against the Standards the program is accredited to.
02
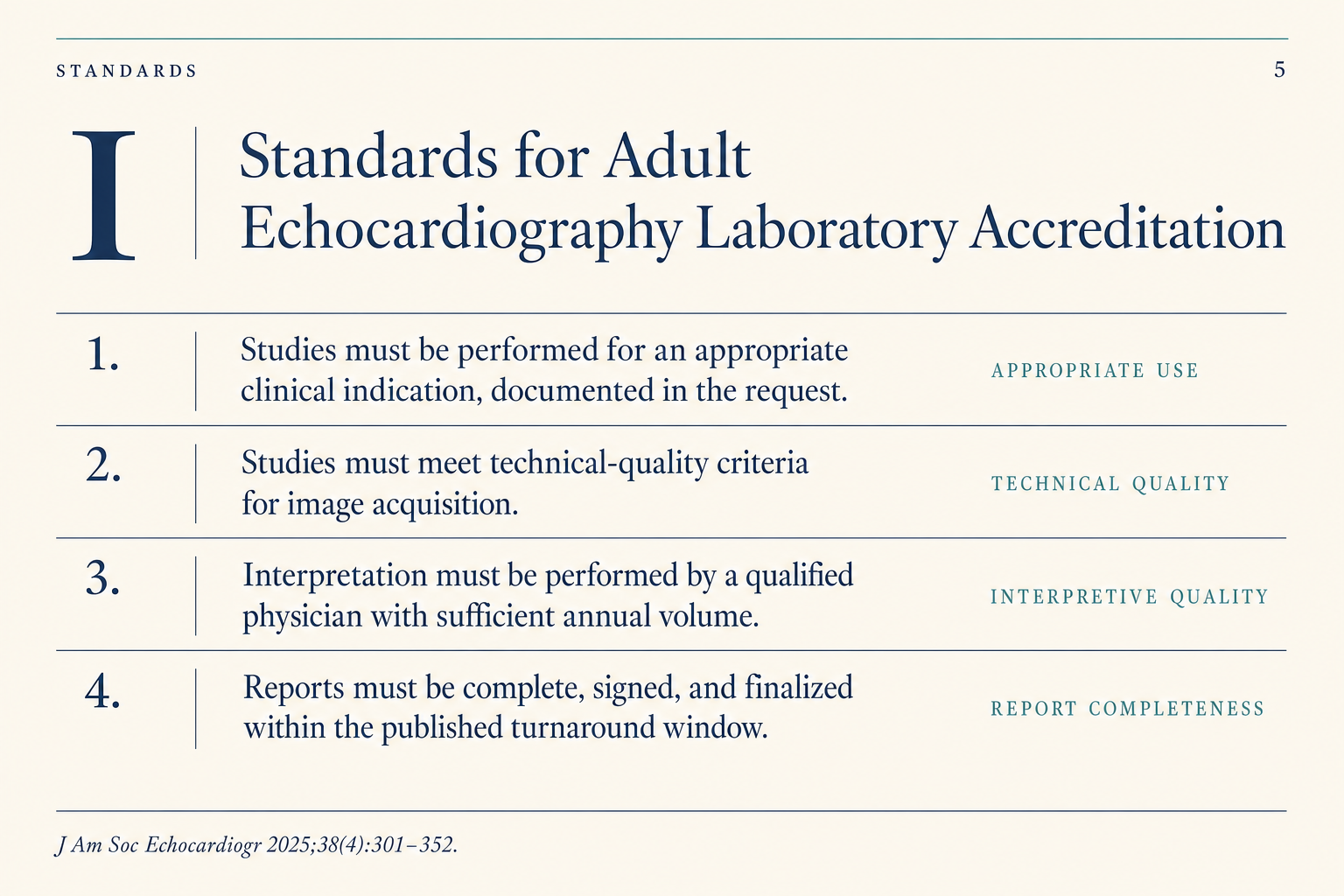
The Standards
The Standards say what the evidence must show. Appropriate use. Technical quality. Interpretive quality. Report completeness and timeliness. Personnel credentials current. Equipment maintained. Volumes met. Many programs carry accreditation as a voluntary quality signal, not a regulatory floor, but a mark a program elects to maintain. The Standards have been refined for decades by the societies that write them. They are not the problem.
The Standards are not the problem.
03
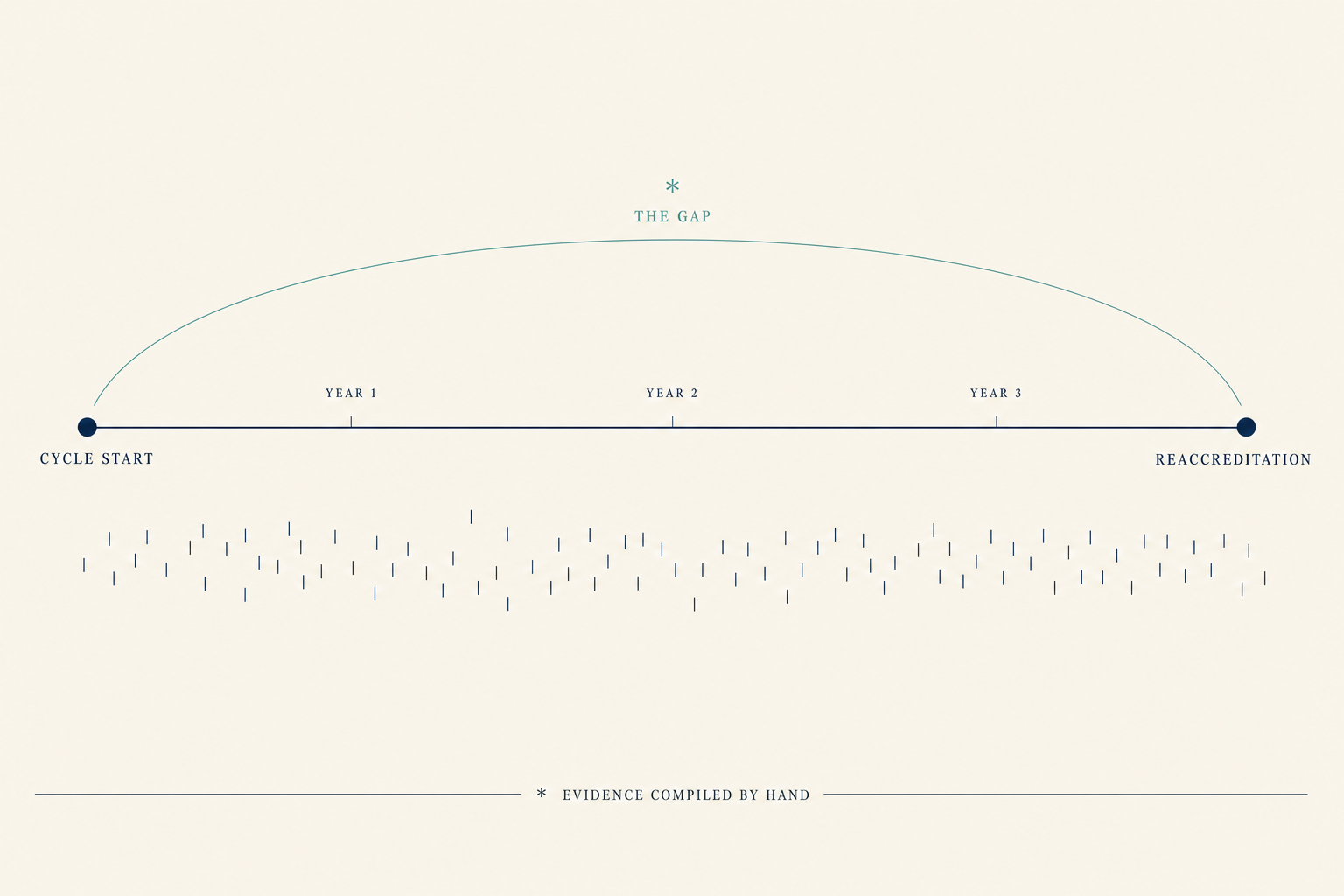
The Gap
The evidence already exists. It sits in the EMR, the credentialing system, and the equipment logs. The gap is that the evidence is compiled by hand once every three years, and nothing watches it in between. Gaps accumulate silently. Renewal arrives as a scramble. Peer reviewers spend their time on completeness, not clinical judgment.
04
The Substrate
Standards encoded as version-controlled rules. FHIR-native pull from the facility's clinical systems. Evidence accumulating continuously against the rule pack for that program area. Findings that cite the clause, the rule version, the metric, and the data the metric was computed from. The cycle becomes continuous because the evidence is continuous. The Standards do not move. The evidence catches up.
The Standards do not move. The evidence catches up.
Compliance evaluation is a deterministic rule engine. The same inputs produce the same finding. Reasoning that proposes actions sits on a separate codebase from the evaluator that judges them. The audit trail does not pass through a model.
Standards-compliant FHIR R4 ingest with code-system mapping for clinical observations. Derived evidence observations are hashed before evaluation. Tested end to end against a public vendor sandbox; production integration is gated on each facility's data-use and information-security review.
The engine has been run against more than one published standards framework. Modality-agnostic. Country-agnostic. New frameworks ship as rule-pack releases, not engine releases.
How the substrate works
Continuous compliance, in five movements.
The same five movements run on every program at every facility, every day. None of them require a surveyor on-site. None of them require a spreadsheet. Every movement writes provenance to the audit trail.
01
Connect
Secure ingest from the facility's clinical systems via FHIR R4. Volumes, reports, credentials, equipment QC, and QI process records read directly. No re-entry, no manual abstraction.
02
Evaluate
Deterministic rule evaluation against the Standards for that program area. No LLM in the compliance path. Same inputs, same finding.
03
Witness
Findings cite the clause, the rule version, the facility-level metric the engine computed, and the dataset window the metric was computed over. The audit surface is the finding.
04
Surface
Facility-side views of the program's compliance posture in near-real time. Accreditor-side views aligned to the Standards the program is accredited to. Sampled case studies surfaced for peer review when the data points to a clause that needs human judgment.
05
Renew
At the cycle boundary, the evidence is already compiled. Reaccreditation becomes a review, not a scramble. Findings that needed remediation between cycles are already closed, with the trail of when and by whom.
Platform
Six layers, one data backbone, one rule engine.
Compliance evaluation belongs next to the clinical data it measures. Clinical data, deterministic compliance evaluation, and reviewer-facing tooling run on a shared substrate, a unified audit model, coordinated role-based access, and one evaluation surface, with protected health information held behind its own storage boundary by design. Standards encoded as code. Evidence accumulating continuously. Findings cite the clause that produced them.
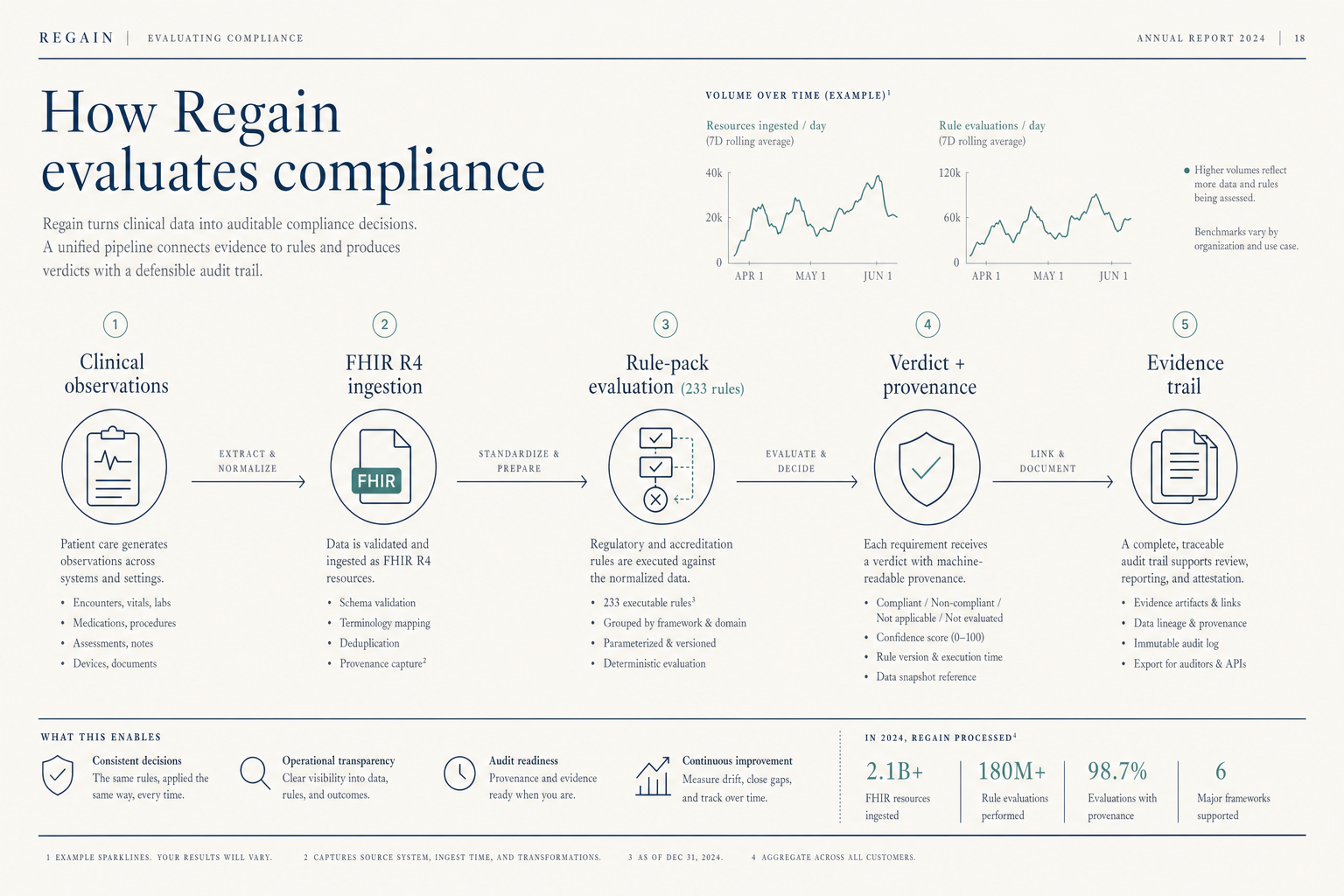
Figure 2.1
How Regain evaluates compliance, end to end
Each finding cites the clause it tests, the rule-pack version that evaluated it, and the facility-level metric the engine computed. Reproducible end to end.
Compliance Engine
Deterministic rule evaluation. The same inputs produce the same finding. No LLM in the compliance path. Findings cite the clause, the rule version, the facility-level metric, and the dataset window the metric was computed over. Reproducible end to end.
FHIR R4-native ingest from the facility's clinical systems. Derived evidence observations are hashed before evaluation. Volumes, reports, credentials, and equipment QC flow into compliance evaluation without manual abstraction.
Reviewer-facing tooling for the work that requires judgment, not completeness checking. Mock surveys against encoded Standards. Gap analysis tied to the underlying metric. Cross-program standards mapping. Reviewers spend their time on what only reviewers can do.
Standards encoded as version-controlled rule packs by program area. Semantic versioning. Priority-based composition. Conflict detection at load time. The engine is fixed; the Standards are configuration. New standards versions ship as rule-pack releases, not engine releases.
Modality- and country-agnostic standards runtime. The engine has been run against more than one published standards framework, with cross-framework mapping where rules overlap.
Each rule traces to an authoritative source through a five-layer hierarchy: regulatory floor, standards from the societies that write them, peer-reviewed evidence, professional guidelines, emerging evidence. Higher layers take precedence. Enforced programmatically.
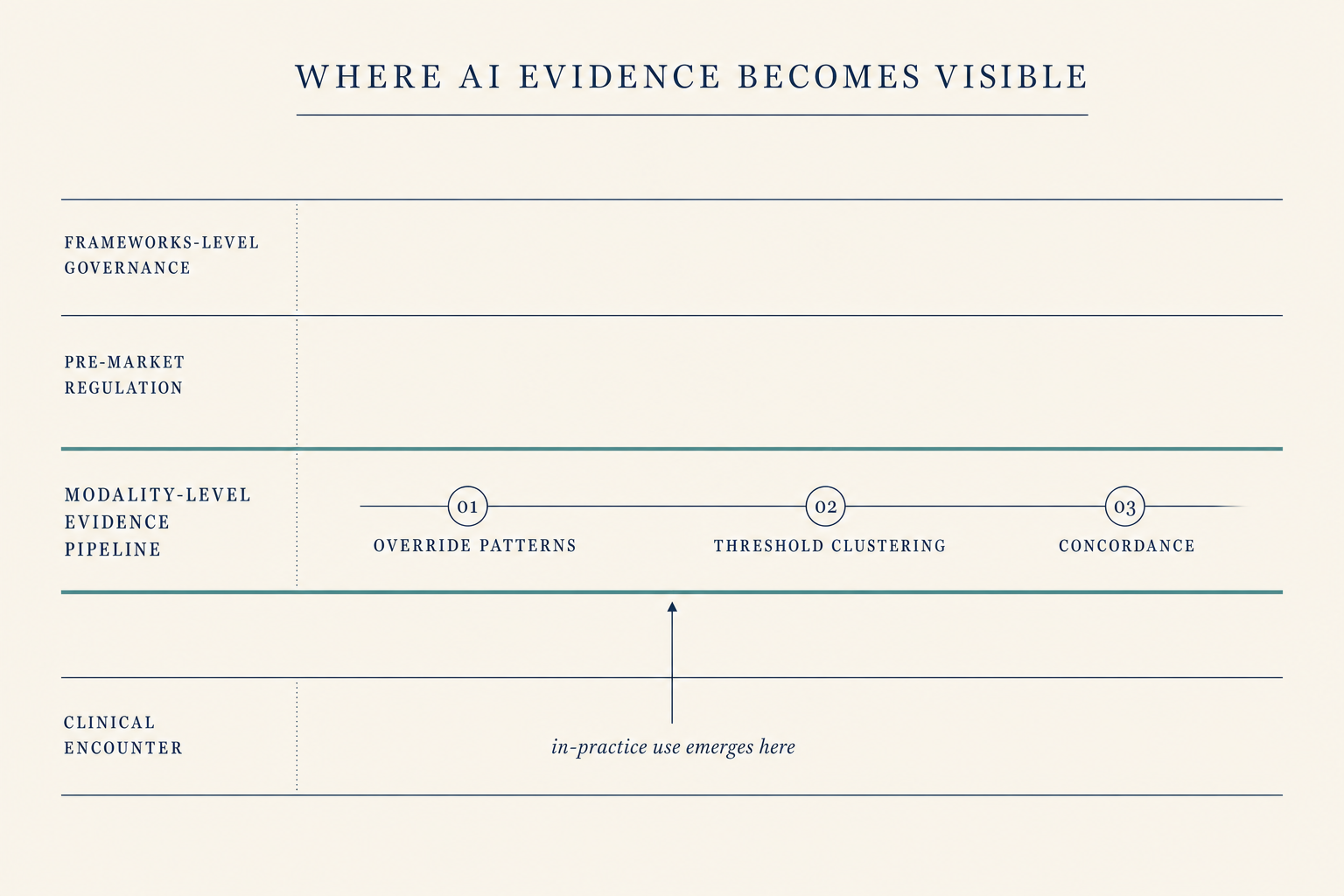
The patterns that show how a tool is actually being used (when measurements get overridden, where thresholds cluster, how AI-suggested values compare to final human readings) emerge from the same evidence pipeline that supports compliance evaluation. The substrate makes those patterns visible. What to do with them is a question for the standards bodies that already define what good practice looks like.
Figure 5.1
Where AI evidence becomes visible
Frameworks-level governance bodies sit at the top. Pre-market regulation sits beneath them. The modality- level evidence pipeline is the band closest to clinical practice, and it is the only band where in-practice use patterns — overrides, threshold clustering, concordance between AI and human readings — become visible. The substrate is the pipeline; what to do with what it surfaces is for the standards body to decide.
Compliance evaluation belongs next to the clinical data it measures, not downstream of it.
When compliance is downstream of the clinical system, an evaluation depends on a chain of integrations, exports, and manual abstractions that stay aligned only if someone is watching them. When compliance is co-resident with the clinical data, evaluation is continuous and automatic, and the compliance posture stays current as the underlying data updates, because the data that drives clinical care is the same data that drives compliance evaluation.
The Standards are not the bottleneck. The evidence pipeline is.
Figure 3.1, Rule-pack decomposition across five program-area packs
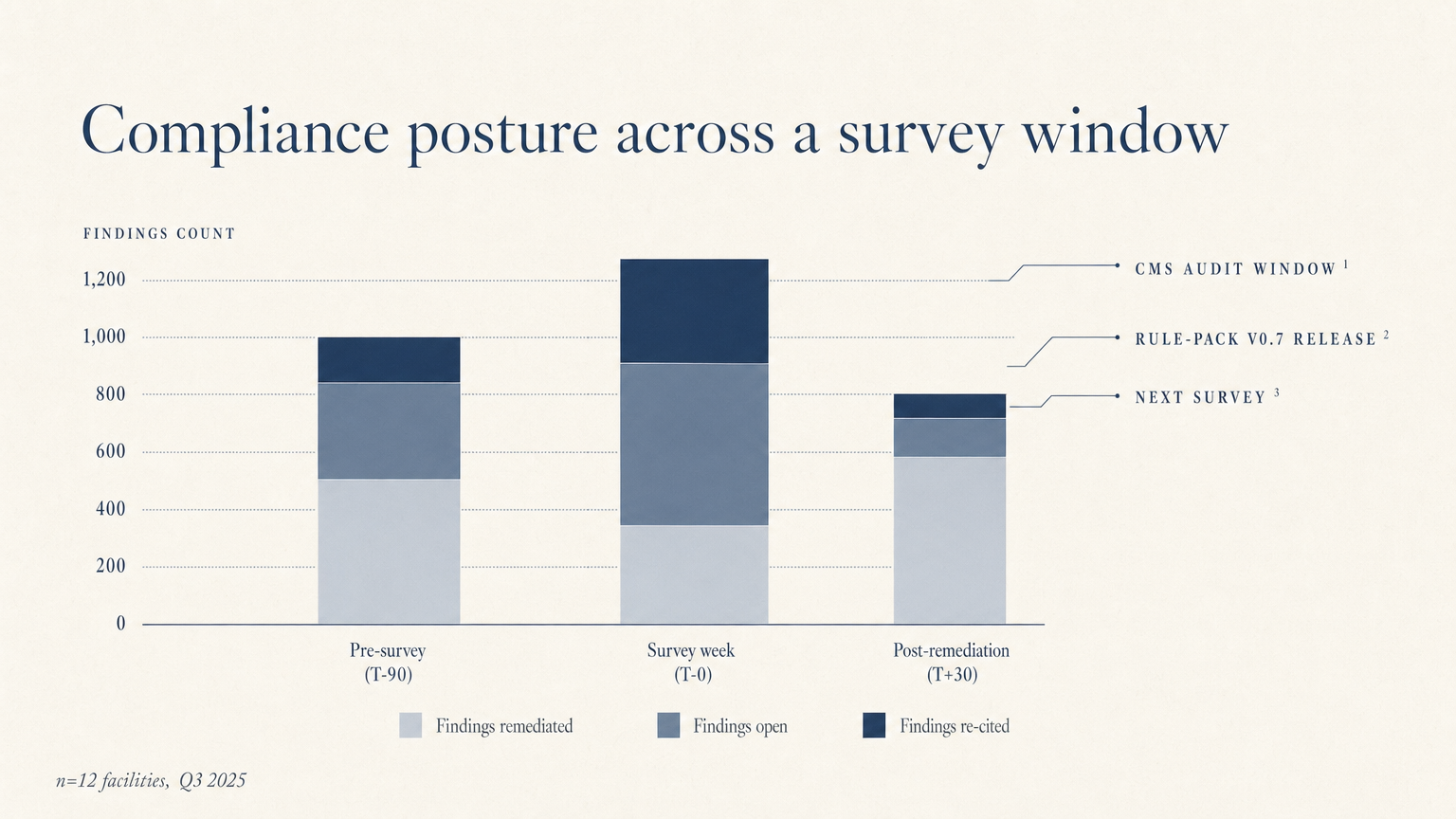
Figure 4.1
Compliance posture across a survey window
Illustrative composite. A program at a facility, scored across a single accreditation cycle. Continuous monitoring closes findings before the survey window; the post-remediation column shows the residual cited findings that drive next-cycle priorities. Not customer data.
Use Cases
Where the visibility gap shows up, and how the substrate closes it.
Eight scenarios drawn from the operational pain of clinical accreditation: between-cycle gap accumulation, manual case sampling, peer-reviewer assignment friction, application completeness failures, equipment QC self-reporting, the slow revision cycle, the silent remediation window, and manual QI documentation. Each scenario is generic; each one is recognizable.
Explore Use Cases →
Insights
Research and analysis on the forces reshaping clinical accreditation.
Long-form pieces from the substrate vantage point: the visibility gap, manual abstraction costs, the voluntary-standards erosion question, the position where AI-use evidence becomes visible, and the transition to continuous monitoring.
Read the Insights →
Trust
How the substrate earns institutional trust.
Deterministic evaluation with no LLM in the compliance path. Structural independence between reasoning and supervision. Open standards where it matters, proprietary depth where it counts. Tooling that frees peer reviewers to spend their time on judgment, not on completeness checking. Building toward HIPAA compliance with an engineered separation of PHI and PII.
See the trust architecture →
About
An infrastructure company. Early in a transformation that will take years.
Regain, Inc. is a Delaware C-Corporation building clinical AI infrastructure for healthcare accreditation. Self-funded. Field experience deploying clinical systems at medical centers in Central Asia. Building toward HIPAA compliance with engineered separation of PHI and PII.
Read about Regain →
See Regain Accreditation in action.
We will walk through your Standards framework and show you what continuous compliance monitoring looks like for the program area you accredit.
Architectural statement, current as of 2026-05-13. The compliance evaluation engine is a deterministic rule evaluator. Reasoning and supervision sit on separate codebases with separate runtimes and separate access controls.
FHIR R4 integration status as of 2026-05-13: end-to-end tested against a public vendor sandbox. Production integration at any specific facility is gated on the facility's institutional data-use agreement and information-security review.
Rule packs encode published standards frameworks. As of 2026-05-13, the engine has been run against more than one publicly available framework. Rule-pack composition spans clinical care, safety and quality, privacy and security, data and interoperability, and operational governance.